Review Article
COVID-19 Vaccines and Variants: Assessing Protection Levels Across Different Strains 
 Author
Author  Correspondence author
Correspondence author
Journal of Vaccine Research, 2024, Vol. 14, No. 5
Received: 25 Jul., 2024 Accepted: 10 Sep., 2024 Published: 20 Sep., 2024
The emergence of various SARS-CoV-2 variants has posed significant challenges to the efficacy of COVID-19 vaccines. This stdy assesses the protection levels offered by different COVID-19 vaccines against multiple SARS-CoV-2 variants, including Alpha (B.1.1.7), Beta (B.1.351), Gamma, and Delta (B.1.617.2). The ChAdOx1 nCoV-19 (AZD1222) vaccine demonstrated reduced neutralization activity against the B.1.1.7 variant but maintained clinical efficacy. Full vaccination with mRNA vaccines showed high effectiveness against the Alpha variant and moderate effectiveness against Beta/Gamma and Delta variants, while partial vaccination was less effective. The BNT162b2 and ChAdOx1 nCoV-19 vaccines exhibited lower effectiveness after one dose against the Delta variant compared to the Alpha variant, but two doses provided substantial protection. The ChAdOx1 nCoV-19 vaccine showed limited efficacy against mild-to-moderate COVID-19 caused by the B.1.351 variant. Overall, while vaccines have significantly reduced the incidence and severity of COVID-19, the emergence of new variants necessitates ongoing evaluation of vaccine efficacy and potential updates to vaccine formulations.
1 Introduction
The COVID-19 pandemic, caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has led to an unprecedented global health crisis. In response, several vaccines have been developed and deployed at an extraordinary pace. Among the most prominent are the mRNA-based vaccines, such as BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna), which have demonstrated high efficacy in preventing symptomatic COVID-19 in clinical trials (Baden et al., 2020; Thompson et al., 2021). These vaccines work by encoding the spike protein of SARS-CoV-2, thereby eliciting an immune response that provides protection against the virus (Mulligan et al., 2020). Other vaccines, including viral vector vaccines like ChAdOx1 (AstraZeneca) and Ad26.COV2.S (Johnson and Johnson), have also been widely used and shown to be effective (Lauring et al., 2022; Zhang et al., 2023).
The emergence of SARS-CoV-2 variants, such as Alpha (B.1.1.7), Beta (B.1.351), Delta (B.1.617.2), and Omicron (B.1.1.529), has raised concerns about the continued efficacy of existing vaccines. These variants have mutations that may affect the virus's transmissibility and its ability to evade the immune response induced by vaccination (Mulligan et al., 2020; Chemaitelly et al., 2021). For instance, the Delta variant has been associated with reduced vaccine effectiveness, necessitating booster doses to maintain high levels of protection (Mulligan et al., 2020). Similarly, the Omicron variant has shown a significant reduction in neutralization by antibodies generated from previous infection or vaccination, although booster doses have been shown to enhance protection (Mulligan et al., 2020; Fiolet et al., 2021). The effectiveness of vaccines against these variants varies, with mRNA vaccines generally showing higher efficacy compared to other types (Haas et al., 2021; Zeng et al., 2021).
This study provides a comprehensive assessment of the protection levels offered by COVID-19 vaccines against different SARS-CoV-2 variants. By synthesizing data from various studies, to understand the extent to which these vaccines remain effective in the face of emerging variants and to identify any gaps in protection that may need to be addressed through booster doses or new vaccine formulations. Understanding the impact of variants on vaccine efficacy is crucial for guiding public health strategies and ensuring that vaccination campaigns remain effective in controlling the pandemic.
2 Overview of COVID-19 Variants
2.1 Emergence of major variants
The COVID-19 pandemic has been marked by the emergence of several significant SARS-CoV-2 variants, each characterized by unique mutations in the spike protein. These mutations have influenced the virus's transmissibility, virulence, and ability to evade immune responses. The World Health Organization (WHO) has classified these variants into categories such as Variants of Concern (VOC), Variants of Interest (VOI), and Variants Under Monitoring (VUM) based on their impact on public health (Thakur et al., 2022).
The first major variant to gain global attention was the D614G mutation, which became predominant worldwide by mid-2020 (Hossain et al., 2021). Following this, four major VOCs were identified: Alpha (B.1.1.7) in the UK, Beta (B.1.351) in South Africa, Gamma (P.1) in Brazil, and Delta (B.1.617.2) in India (Tao et al., 2021). These variants share several mutations, particularly in the spike protein, which have been linked to increased transmissibility and potential immune escape (Hossain et al., 2021; Tao et al., 2021).
2.2 Immune evasion mechanisms
SARS-CoV-2 variants have developed various mechanisms to evade the immune system, complicating efforts to control the pandemic through vaccination and therapeutic interventions. The spike protein mutations, particularly in the receptor-binding domain (RBD), play a crucial role in immune evasion. For instance, the E484K mutation found in the Beta and Gamma variants significantly reduces the neutralization capacity of antibodies from convalescent plasma and vaccinated individuals (Hoffmann et al., 2021; Wang et al., 2021).
The Beta variant (B.1.351) is notably resistant to neutralization by most monoclonal antibodies targeting the N-terminal domain (NTD) and RBD, largely due to the E484K mutation (Wang et al., 2021). Similarly, the Gamma variant (P.1) also exhibits resistance to neutralizing antibodies, which poses challenges for monoclonal antibody therapies and vaccine efficacy (Hoffmann et al., 2021). The Delta variant (B.1.617.2) has shown reduced susceptibility to neutralization by sera from vaccinated individuals, indicating the need for continuous monitoring and potential updates to vaccine formulations (Lazarević et al., 2021).
2.3 Global spread and its impact
The global spread of these variants has had profound implications for public health measures, vaccine efficacy, and the overall trajectory of the pandemic. The Alpha variant (B.1.1.7) demonstrated a higher transmissibility rate, leading to its rapid spread across more than 50 countries and necessitating stricter public health measures (Hossain et al., 2021). The Beta variant (B.1.351) and Gamma variant (P.1) have also spread internationally, albeit to a lesser extent, but their ability to evade immune responses has raised significant concerns (Hossain et al., 2021).
The Delta variant (B.1.617.2) has been particularly impactful, becoming the dominant strain in many regions due to its high transmissibility and partial resistance to neutralization by antibodies (Lazarević et al., 2021). This variant's spread has led to increased infection rates, hospitalizations, and deaths, even in populations with high vaccination coverage (Lazarević et al., 2021). The emergence of new variants such as the New York variant (B.1.526) and the California variant (B.1.427/B.1.429) further underscores the dynamic nature of the virus and the ongoing need for vigilant surveillance and adaptive public health strategies (Hossain et al., 2021; Xu and Li, 2024).
The emergence and spread of SARS-CoV-2 variants have significantly influenced the course of the COVID-19 pandemic. These variants have introduced new challenges in terms of increased transmissibility, immune evasion, and the need for continuous updates to vaccines and therapeutic approaches. Ongoing research and global cooperation are essential to address these challenges and mitigate the impact of current and future variants on public health.
3 Vaccine Effectiveness Against Variants
3.1 Protection against Alpha variant
The Alpha variant (B.1.1.7) was one of the first variants of concern to emerge, leading to significant global spread. Studies have shown that the initial COVID-19 vaccines provided robust protection against this variant. For instance, a study conducted in the United States demonstrated that mRNA vaccines were highly effective in preventing hospital admissions due to the Alpha variant, with an effectiveness rate of 85% after two doses (Lauring et al., 2022). Similarly, a Danish nationwide cohort study reported a vaccine effectiveness (VE) of 90.7% against Alpha infection 14 to 30 days post-vaccination, which waned to 73.2% after more than 120 days (Gram et al., 2022). These findings underscore the high initial effectiveness of the vaccines against the Alpha variant, although a gradual decline in protection over time was observed.
3.2 Effectiveness against delta variant
The Delta variant (B.1.617.2) posed a more significant challenge due to its higher transmissibility and partial immune escape capabilities. Vaccine effectiveness against the Delta variant was generally lower compared to the Alpha variant but still substantial. In the United States, mRNA vaccines showed an effectiveness of 85% against hospital admissions after two doses, which increased to 94% after a third dose (Lauring et al., 2022). A study in England found that vaccine effectiveness against symptomatic disease caused by the Delta variant was 65.5% after two doses of the BNT162b2 (Pfizer-BioNTech) vaccine, dropping to 8.8% at 25 or more weeks post-vaccination. However, a booster dose significantly increased protection, with effectiveness rising to 67.2% shortly after the booster (Andrews et al., 2022).
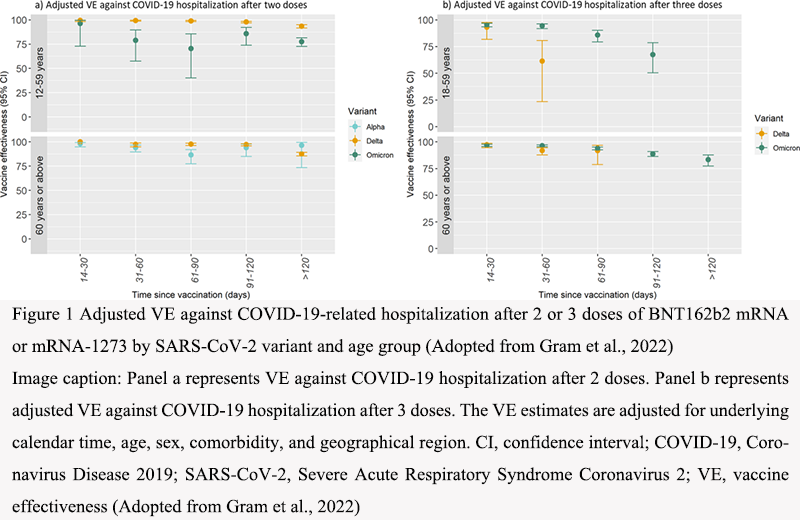
In Denmark, the VE against Delta infection was 82.3% shortly after vaccination, decreasing to 50.0% after more than 120 days. The third dose substantially increased protection, with VE estimates of 86.1% against Delta infection 14 to 30 days post-vaccination (Figure 1) (Gram et al., 2022). These results highlight the importance of booster doses in maintaining high levels of protection against the Delta variant.
|
Figure 1 Adjusted VE against COVID-19-related hospitalization after 2 or 3 doses of BNT162b2 mRNA or mRNA-1273 by SARS-CoV-2 variant and age group (Adopted from Gram et al., 2022) Image caption: Panel a represents VE against COVID-19 hospitalization after 2 doses. Panel b represents adjusted VE against COVID-19 hospitalization after 3 doses. The VE estimates are adjusted for underlying calendar time, age, sex, comorbidity, and geographical region. CI, confidence interval; COVID-19, Coronavirus Disease 2019; SARS-CoV-2, Severe Acute Respiratory Syndrome Coronavirus 2; VE, vaccine effectiveness (Adopted from Gram et al., 2022) |
3.3 Effectiveness against Omicron variant
The Omicron variant (B.1.1.529) has presented the most significant challenge to vaccine effectiveness due to its extensive mutations, particularly in the spike protein, which have led to increased immune evasion. Initial studies indicated that the primary vaccination series provided limited protection against Omicron infection. For example, a systematic review found that the protection from primary vaccination against Omicron infection was inferior to that against Delta and Alpha infections, with effectiveness waning faster over time (Paul et al., 2023). Another study reported that vaccine effectiveness against symptomatic disease caused by Omicron was only 65% shortly after two doses, dropping to 8.8% at 25 or more weeks (Andrews et al., 2022).
However, booster doses have been shown to significantly improve protection against Omicron. A Danish study reported that the third dose increased VE against Omicron infection to 57.7% shortly after the booster, although this protection also waned over time (Gram et al., 2022). Similarly, a meta-analysis found that a booster dose restored protection against Omicron infection up to 51.1% within three months, although this waned to 32.8% within six months (Mohammed et al., 2023). Despite the reduced effectiveness against infection, vaccines have maintained high effectiveness against severe outcomes. For instance, the VE against Omicron-associated hospitalization remained high, with estimates of 95.5% or above shortly after vaccination (Gram et al., 2022).
While the primary vaccination series provides limited and short-lived protection against Omicron infection, booster doses significantly enhance and prolong protection. However, the effectiveness of these boosters also wanes over time, indicating the potential need for regular booster doses to maintain high levels of immunity against the Omicron variant.
4 The Waning of Vaccine Protection and the Efficacy of Booster Shots
4.1 Waning vaccine efficacy
The efficacy of COVID-19 vaccines has been shown to decline over time, a phenomenon observed across various vaccine types and populations. Studies have consistently reported a significant reduction in antibody levels and vaccine effectiveness within months following the completion of the primary vaccination series. For instance, a systematic review highlighted that the peak humoral response is typically reached 21-28 days after the second dose of mRNA vaccines, after which antibody levels progressively diminish. By 4-6 months post-vaccination, there is a notable decline in both anti-receptor binding domain immunoglobulin G (IgG) and anti-spike IgG levels, with reductions ranging from 55% to 95% depending on the time frame and specific antibody measured (Notarte et al., 2021).
This waning immunity is not limited to mRNA vaccines. Similar trends have been observed with other vaccine platforms, including inactivated vaccines. For example, a study on the BBIBP-CorV vaccine reported a significant decrease in antibody levels three months after the second dose, underscoring the need for booster doses to maintain adequate protection (Chansaenroj et al., 2022). The decline in vaccine efficacy is particularly concerning in the context of emerging variants of concern (VOCs) such as Delta and Omicron, which have shown the ability to partially evade immunity conferred by the initial vaccination series (Menegale et al., 2023).
4.2 Immune response mechanism of boosters
Booster doses are designed to reinvigorate the immune system by enhancing both humoral and cellular responses. The administration of a booster dose has been shown to significantly increase neutralizing antibody titers against SARS-CoV-2, including its variants. For instance, a meta-analysis demonstrated that the first booster dose of COVID-19 vaccines could induce higher seroconversion rates and neutralizing antibody titers compared to the full vaccination series, thereby providing robust cellular immune responses (Xu et al., 2023).
The mechanism behind this enhanced response involves the reactivation of memory B cells and T cells, which are crucial for long-term immunity. Boosters help in generating a more potent and durable immune response by increasing the quantity and quality of antibodies. This is particularly important for older adults, who may have a weaker initial response to vaccination. A study comparing homologous and heterologous mRNA vaccine boosters found that heterologous boosters (e.g., BNT162b2 followed by mRNA-1273) induced a stronger neutralizing response against the Omicron variant, especially in older individuals (Poh et al., 2022).
4.3 Clinical effects of boosters
The clinical benefits of booster doses are evident in their ability to reduce the risk of SARS-CoV-2 infection and severe COVID-19 outcomes. A comprehensive meta-analysis revealed that individuals who received a booster dose had significantly lower risks of infection, ICU admission, and death compared to those who only completed the primary vaccination series. The risk ratios for these outcomes were markedly lower in the booster group, indicating the substantial protective effect of booster doses (Xu et al., 2023).
Moreover, booster doses have been shown to enhance protection against various VOCs. For example, a study on the inactivated COVID-19 vaccine BBV152 (Covaxin) reported that a third dose significantly elevated neutral
5 Case Studies of Vaccine Effectiveness Against Variants
5.1 Case study 1: vaccine effectiveness in the U.S. against alpha and delta variants
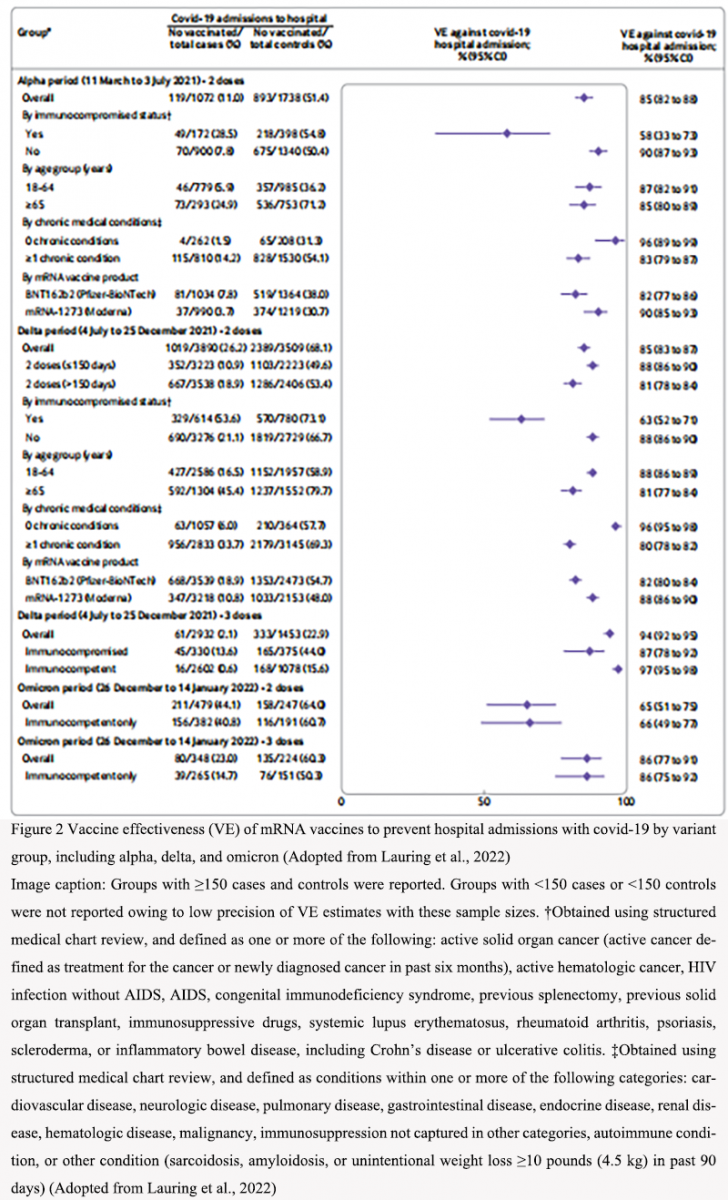
In the United States, the effectiveness of COVID-19 vaccines against the Alpha (B.1.1.7) and Delta (B.1.617.2) variants has been extensively studied. The mRNA vaccines, particularly BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna), have shown high efficacy against these variants. A study conducted across 21 hospitals in the U.S. found that two doses of mRNA vaccines were 85% effective in preventing hospital admissions due to the Alpha variant and 85% effective against the Delta variant. However, the effectiveness against the Delta variant increased to 94% with a third dose (Figure 2) (Lauring et al., 2022).
|
Figure 2 Vaccine effectiveness (VE) of mRNA vaccines to prevent hospital admissions with covid-19 by variant group, including alpha, delta, and omicron (Adopted from Lauring et al., 2022) Image caption: Groups with ≥150 cases and controls were reported. Groups with <150 cases or <150 controls were not reported owing to low precision of VE estimates with these sample sizes. †Obtained using structured medical chart review, and defined as one or more of the following: active solid organ cancer (active cancer defined as treatment for the cancer or newly diagnosed cancer in past six months), active hematologic cancer, HIV infection without AIDS, AIDS, congenital immunodeficiency syndrome, previous splenectomy, previous solid organ transplant, immunosuppressive drugs, systemic lupus erythematosus, rheumatoid arthritis, psoriasis, scleroderma, or inflammatory bowel disease, including Crohn’s disease or ulcerative colitis. ‡Obtained using structured medical chart review, and defined as conditions within one or more of the following categories: cardiovascular disease, neurologic disease, pulmonary disease, gastrointestinal disease, endocrine disease, renal disease, hematologic disease, malignancy, immunosuppression not captured in other categories, autoimmune condition, or other condition (sarcoidosis, amyloidosis, or unintentional weight loss≥10 pounds (4.5 kg) in past 90 days) (Adopted from Lauring et al., 2022) |
.png)
.png){kind=link}
{kind=link}
Another study highlighted that the effectiveness of two doses of the BNT162b2 vaccine was 93.7% against the Alpha variant and 88.0% against the Delta variant. For the ChAdOx1 nCoV-19 (AstraZeneca) vaccine, the effectiveness was 74.5% against the Alpha variant and 67.0% against the Delta variant (Bernal et al., 2021). These findings underscore the importance of full vaccination, as partial vaccination was significantly less effective, with VE of 59.0% against Alpha and 52.6% against Delta (Zeng et al., 2021).
5.2 Case study 2: vaccine efficacy in South Africa against the beta variant
In South Africa, the Beta (B.1.351) variant posed significant challenges due to its ability to partially evade immune responses. The efficacy of various vaccines against this variant has been variable. For instance, the ChAdOx1 nCoV-19 (AstraZeneca) vaccine showed an efficacy of only 10.4% in preventing mild to moderate COVID-19 caused by the Beta variant (Fiolet et al., 2021). In contrast, the NVX-CoV2373 (Novavax) vaccine demonstrated an efficacy of 50% in South Africa, where the Beta variant was dominant (Fiolet et al., 2021).
A systematic review and meta-analysis reported that full vaccination with mRNA vaccines provided moderate effectiveness against the Beta variant, with a VE of 70.7% (Zeng et al., 2021). This was corroborated by seroneutralization studies, which showed a significant reduction in neutralizing activity against the Beta variant for mRNA vaccines, Sputnik V, and CoronaVac (Fiolet et al., 2021). Despite these challenges, full immunization with mRNA vaccines was effective in preventing severe outcomes, including hospitalization and death, even against the Beta variant (Fiolet et al., 2021).
5.3 Case study 3: vaccine effectiveness in denmark against the Omicron variant
Denmark has been at the forefront of monitoring the effectiveness of COVID-19 vaccines against the Omicron (B.1.1.529) variant. A nationwide cohort study in Denmark revealed that two doses of mRNA vaccines provided limited and short-lived protection against Omicron infection, with a VE of only 39.9% shortly after vaccination, which waned to 4.4% over time (Gram et al., 2022). However, the effectiveness against COVID-19 hospitalization remained high, with VE estimates of 95.5% or above for Omicron after two or three doses (Gram et al., 2022).
The study also highlighted the importance of booster doses. The third dose of mRNA vaccines significantly increased protection against Omicron infection, with a VE of 57.7% shortly after the booster dose (Gram et al., 2022). This aligns with findings from other studies, which reported that mRNA vaccine boosters reestablished effectiveness against Omicron, although to a lower extent compared to Delta and Alpha variants (Paul et al., 2023).
6 Comparison of Different Vaccine Types
6.1 mRNA vaccines: the performance of BNT162b2 and moderna against different variants
mRNA vaccines, particularly BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna), have shown varying levels of effectiveness against different SARS-CoV-2 variants. During the Delta variant predominance, the effectiveness of two doses of mRNA vaccines against COVID-19-associated emergency department (ED) and urgent care (UC) encounters was 86% within 14-179 days post-vaccination, dropping to 76% after 180 days. However, a third dose significantly boosted effectiveness to 94% (Thompson et al., 2022). Against the Omicron variant, the effectiveness of two doses dropped substantially to 52% within 14-179 days and 38% after 180 days, but a third dose increased effectiveness to 82% (Thompson et al., 2022). This pattern was also observed in hospitalizations, where the effectiveness of two doses against Delta was 90% within 14-179 days and 81% after 180 days, while a third dose increased it to 94%. For Omicron, the effectiveness was 81% within 14-179 days and 57% after 180 days, with a third dose boosting it to 90% (Thompson et al., 2022).
A systematic review and meta-analysis further confirmed that booster doses of mRNA vaccines provide better protection against Omicron infections compared to the full dose. The booster dose showed a 22% increase in protection against any Omicron infection, 20% against severe infections, and 22% against symptomatic infections within three months (Pratama et al., 2022). However, the effectiveness of the booster dose also waned over time, indicating the need for regular booster shots to maintain high levels of protection (Pratama et al., 2022).
6.2 Inactivated vaccines: protection levels against omicron
Inactivated vaccines, such as CoronaVac (Sinovac), have shown lower effectiveness against the Omicron variant compared to mRNA vaccines. Studies have indicated that two-dose regimens of inactivated vaccines induce low to negligible neutralizing antibodies (NAb) against Omicron (Niyomnaitham et al., 2022). However, a booster dose of an mRNA vaccine following a primary series of inactivated vaccines significantly increased the NAb titers against Omicron, suggesting that heterologous booster regimens could enhance protection (Niyomnaitham et al., 2022).
A systematic review highlighted that the protection from primary vaccination with inactivated vaccines against Omicron infection is inferior to that against Delta and Alpha infections and wanes faster over time. However, primary vaccination still preserved strong protection against Omicron-associated hospitalization, severity, and death, even months after the last dose. Boosters provided more robust and longer-lasting protection against hospitalizations due to Omicron compared to the primary series alone (Paul et al., 2023).
6.3 Adenovirus vector vaccines: efficacy of the ChAdOx1 vaccine against various strains
Adenovirus vector vaccines, such as ChAdOx1 (AstraZeneca), have demonstrated robust immune responses, although they elicit lower antibody responses compared to mRNA vaccines. Despite this, they are nearly as effective in preventing severe disease, likely due to the generation of immune memory cells (Fryer et al., 2023). Studies have shown that ChAdOx1 vaccination elicits a strong memory B cell response capable of recognizing Omicron subvariants BA.2 and BA.5. The second dose of ChAdOx1 boosted memory B cells that recognized variants of concern (VoC), with 37% and 39% of Wuhan-Hu-1-specific memory B cells recognizing BA.2 and BA.5, respectively (Fryer et al., 2023).
A systematic review and meta-analysis found that the effectiveness of ChAdOx1 against Omicron infection was moderate, but a booster dose provided better protection against severe infection. The effectiveness of the booster dose against severe Omicron infections was 18% within three months and 37% for symptomatic infections (Pratama et al., 2022; Li, 2024). This suggests that while the primary series of ChAdOx1 provides some level of protection, booster doses are crucial for maintaining higher levels of effectiveness against emerging variants.
While mRNA vaccines like BNT162b2 and Moderna have shown high effectiveness against various SARS-CoV-2 variants, including Delta and Omicron, their protection wanes over time, necessitating booster doses. Inactivated vaccines offer lower initial protection against Omicron but can be significantly enhanced with mRNA boosters. Adenovirus vector vaccines like ChAdOx1 provide robust immune memory responses, and their effectiveness can also be improved with booster doses. Regular booster vaccinations are essential to maintain high levels of protection against COVID-19 across different vaccine types and variants (Pratama et al., 2022; Thompson et al., 2022; Niyomnaitham et al., 2022; Fryer et al., 2023; Paul et al., 2023).
7 Development and Future Prospects of Next-Generation Vaccines
7.1 New vaccines targeting variants
The rapid emergence of SARS-CoV-2 variants has necessitated the development of vaccines specifically targeting these new strains. Recent studies have shown that vaccines based on the ancestral spike protein may not provide sufficient protection against newer variants such as Omicron and its sub-lineages (Kang et al., 2023). To address this, researchers have developed multivalent vaccines using platforms like the Ad5/35 vector, which encode spike proteins from multiple variants. These vaccines have demonstrated the ability to induce broadly neutralizing antibodies, thereby offering enhanced protection against a range of circulating strains (Kang et al., 2023).
Moreover, mRNA technology has proven to be highly adaptable for rapid vaccine development. For instance, an mRNA vaccine encoding a trimeric receptor-binding domain (RBD) fused to ferritin nanoparticles has shown robust and durable immune responses in preclinical studies. This vaccine was quickly modified to target specific variants, producing broad-spectrum neutralizing antibodies against both Alpha and Beta variants (Sun et al., 2021). Such advancements highlight the potential for mRNA vaccines to be swiftly updated to combat emerging variants.
7.2 Potential of broad-spectrum vaccines
The development of broad-spectrum vaccines is crucial for providing protection against multiple SARS-CoV-2 variants and future viral mutations. Broad-spectrum vaccines aim to induce immunity that is effective across a wide range of viral strains, reducing the need for frequent updates. One promising approach involves the use of chimeric RBD constructs from different coronaviruses. For example, a DNA vaccine encoding a dimeric RBD chimera of SARS-CoV-1 and SARS-CoV-2 variants has shown potent immunogenicity and broad-spectrum protection in preclinical models (Fan et al., 2023). This vaccine, delivered via microneedle array patches, elicited strong neutralizing antibody responses and protected mice from Omicron BA.1 challenge.
Additionally, the development of polyvalent vaccines, which include antigens from multiple variants, has shown promise. A bivalent vaccine combining antigens from BA.5 and BA.2.75 variants induced broadly neutralizing antibodies and improved cross-neutralization capacity in preclinical studies (Kang et al., 2023). Such vaccines could provide a more comprehensive immune response, potentially reducing the impact of future variants.
7.3 Prospects of mRNA technology and other innovative platforms
mRNA technology has revolutionized vaccine development, offering rapid and flexible solutions to emerging infectious diseases. The success of mRNA vaccines like Pfizer/BioNTech's BNT162b2 and Moderna's mRNA-1273 has demonstrated the potential of this platform to provide high levels of protection against COVID-19 (Sharif et al., 2021; Rudan et al., 2022). The ability to quickly modify mRNA sequences to target new variants makes this technology particularly valuable in the ongoing fight against SARS-CoV-2.
Innovative platforms such as viral vectors and nanotechnology are also being explored for next-generation vaccines. For instance, adenoviral vector-based vaccines have shown efficacy in inducing strong immune responses and can be engineered to target multiple variants (Kang et al., 2023). Additionally, nanoparticle-based vaccines, such as those using ferritin-formed nanoparticles, have demonstrated the ability to enhance the stability and immunogenicity of vaccine antigens (Sun et al., 2021).
The integration of these innovative platforms with traditional vaccine approaches could lead to the development of vaccines that are not only effective against current variants but also adaptable to future mutations. For example, the use of self-assembled nanoparticle-based trimeric RBD mRNA vaccines has shown promise in providing broad-spectrum protection and could serve as a reference for future vaccine design (Sun et al., 2021).
8 Concluding Remarks
The evolution of COVID-19 vaccines has been a dynamic process, driven by the emergence of new variants that challenge the efficacy of existing vaccines. Initially, vaccines were developed based on the ancestral strain of SARS-CoV-2, which provided substantial protection against severe disease and symptomatic infection. However, as the virus evolved, new variants such as Delta and Omicron emerged, each with mutations that allowed them to partially evade the immune response elicited by these vaccines.
The Omicron variant, in particular, has posed significant challenges due to its high transmissibility and numerous mutations in the spike protein. Studies have shown that while the original vaccines still offer protection against severe disease, their efficacy against symptomatic infection has decreased. This has led to the development of multivalent and bivalent vaccines designed to target multiple variants simultaneously. For instance, vaccines based on the adenovirus type 5/35 vector platform have been developed to include spike proteins from various Omicron subvariants, showing promising results in broadening immunity.
The waning immunity observed over time and the continuous emergence of new variants underscore the importance of booster doses. Booster vaccinations have been shown to significantly enhance neutralizing antibody levels, thereby improving protection against both existing and emerging variants. For example, heterologous booster regimens, which combine different types of vaccines, have demonstrated superior immunogenicity compared to homologous boosters, particularly in older adults.
Future vaccine strategies must focus on developing vaccines that can provide broad and durable protection. This includes the creation of next-generation multivalent vaccines that can target a wide array of variants. Additionally, the timely updating of booster vaccines to include antigens from newly circulating variants is crucial. Research is also exploring alternative delivery methods, such as inhalation, to enhance mucosal immunity, which could provide an additional layer of protection against respiratory viruses like SARS-CoV-2.
While the initial COVID-19 vaccines have been instrumental in reducing the severity of the pandemic, the ongoing evolution of the virus necessitates continuous adaptation of vaccine strategies. Boosters play a critical role in maintaining high levels of immunity, and future vaccines must be designed to offer broad and long-lasting protection against a diverse range of variants. The collaborative efforts of the global scientific community will be essential in achieving these goals and ultimately controlling the spread of COVID-19.
Acknowledgments
The author extends sincere thanks to two anonymous peer reviewers for their feedback on the manuscript.
Conflict of Interest Disclosure
The author affirms that this research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
Andrews N., Stowe J., Kirsebom F., Toffa S., Rickeard T., Gallagher E., Gower C., Kall M., Groves N., O’Connell A.M., Simons D., Blomquist P.B., Zaidi A., Nash S., Aziz N.I.B.A., Thelwall S., Dabrera G., Myers R., Amirthalingam G., Gharbia S., Barrett J.C., Elson R., Ladhani S.N., Ferguson N., Zambon M., Campbell C.N.J., Brown K., Hopkins S., Chand M., Ramsay M., and Bernal J.L., 2022, Covid-19 vaccine effectiveness against the Omicron (B.1.1.529) variant, The New England Journal of Medicine, 386(16): 1532-1546.
https://doi.org/10.1056/NEJMoa2119451
PMID: 35249272 PMCID: PMC8908811
Baden L.R., Sahly H.M.E., Essink B., Kotloff K., Frey S., Novak R., Diemert D., Spector S.A., Rouphael N., Creech C.B., Mcgettigan J., Kehtan S., Segall N., Solis J., Brosz A., Fierro C., Schwartz H., Neuzil K., Corey L., Gilbert P., Janes H., Follmann D., Marovich M., Mascola J., Polakowski L., Ledgerwood J., Graham B.S., Bennett H., Pajon R., Knightly C., Leav B., Deng W., Zhou H.H., Han S., Ivarsson M., Miller J., Zaks T., and COVE Study Group, 2020, Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine, The New England Journal of Medicine, 384(5): 403-416.
https://doi.org/10.1056/NEJMoa2035389
PMID: 33378609 PMCID: PMC7787219
Bernal J.L., Andrews N., Gower C., Gallagher E., Simmons R., Thelwall S., Stowe J., Tessier E., Groves N., Dabrera G., Myers R., Campbell C.N.J., Amirthalingam G., Edmunds M., Zambon M., Brown K., Hopkins S., Chand M., and Ramsay M., 2021, Effectiveness of Covid-19 vaccines against the B.1.617.2 (Delta) variant, The New England Journal of Medicine, 385(7): 585-594.
https://doi.org/10.1056/NEJMoa2108891
PMID: 34289274 PMCID: PMC8314739
Chansaenroj, J., Suntronwong, N., Kanokudom, S., Assawakosri, S., Yorsaeng, R., Vichaiwattana, P., Klinfueng, S., Wongsrisang, L., Srimuan, D., Thatsanatorn, T., Thongmee, T., Auphimai, C., Nilyanimit, P., Wanlapakorn, N., Sudhinaraset, N., and Poovorawan, Y., 2022, Immunogenicity following two doses of the BBIBP-CorV vaccine and a third booster dose with a viral vector and mRNA COVID-19 vaccines against delta and omicron variants in prime immunized adults with two doses of the BBIBP-CorV vaccine, Vaccines, 10(7): 1071.
https://doi.org/10.3390/vaccines10071071
PMID: 35891235 PMCID: PMC9317843
Chemaitelly H., Yassine H.M., Benslimane F.M., Khatib H.A.A, Tang, P., Hasan M.R., Malek J.A., Coyle P., Ayoub H.H., Kanaani Z.A., Kuwari E.A., Jeremijenko A., Kaleeckal A.H., Latif A.N., Shaik R.M., Rahim H.F,A., Nasrallah G.K., Kuwari M.G.A., Romaih, H.E.A., Al-Thani, M.H., Kha, A.A., Butt A.A., Bertollini R., and Abu-Raddad L.J., 2021, mRNA-1273 COVID-19 vaccine effectiveness against the B.1.1.7 and B.1.351 variants and severe COVID-19 disease in Qatar, Nature Medicine, 27(9): 1614-1621.
https://doi.org/10.1038/s41591-021-01446-y
Fan F., Zhang X., Zhang Z.Y., Ding Y., Wang L.M., Xu X., Pan Y.Y., Gong F.Y., Jiang L., Kang L.Y., Ha Z., Lu H.J., Hou J.W., Kou Z.H., Zhao G., Wang B., and Gao X.M., 2023, Potent immunogenicity and broad-spectrum protection potential of microneedle array patch-based COVID-19 DNA vaccine candidates encoding dimeric RBD chimera of SARS-CoV and SARS-CoV-2 variants, Emerging Microbes and Infections, 12(1): 2202269.
https://doi.org/10.1080/22221751.2023.2202269
PMID: 37038652 PMCID: PMC10155640
Fiolet T., Kherabi Y., MacDonald C., Ghosn J., and Peiffer-Smadja N., 2021, Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: a narrative review, Clinical Microbiology and Infection, 28(2): 202-221.
https://doi.org/10.1016/j.cmi.2021.10.005
PMID: 34715347 PMCID: PMC8548286
Fryer H.A., Hartley, G.E., Edwards, E.S.J., Varese N., Boo I., Bornheimer S.J., Hogarth P.M., Drummer H.E., O’Hehir R.E., and van Zelm M.C., 2023, COVID-19 adenoviral vector vaccination elicits a robust memory b cell response with the capacity to recognize Omicron BA.2 and BA.5 variants, Journal of Clinical Immunology, 43(7): 1506-1518.
https://doi.org/10.1007/s10875-023-01527-2
PMID: 37322095 PMCID: PMC10499924
Gram M.A., Emborg H.D., Schelde A.B., Friis N.U., Nielsen K.F., Moustsen-Helms I.R., Legarth R., Lam J.U.H., Chaine M., Malik A.Z., Rasmussen M., Fonager J., Sieber R.N., Stegger M., Ethelberg S., Valentiner-Branth P., and Hansen C.H., 2022, Vaccine effectiveness against SARS-CoV-2 infection or COVID-19 hospitalization with the Alpha, Delta, or Omicron SARS-CoV-2 variant: a nationwide danish cohort study, PLoS Medicine, (9): e1003992.
https://doi.org/10.1371/journal.pmed.1003992
PMID: 36048766 PMCID: PMC9436060
Haas E.J., Angulo F.J., McLaughlin J.M., Anis E., Singer S.R., Khan F., Brooks N., Smaja M., Mircus G., Pan K., Southern J., Swerdlow D., Jodar L., Levy Y., and Alroy-Preis S., 2021, Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data, Lancet (London, England), 397(10287): 1819-1829.
https://doi.org/10.1016/S0140-6736(21)00947-8
PMID: 33964222 PMCID: PMC8099315
Hoffmann M., Arora P., Gross R., Seidel A., Hörnich B., Hahn A., Krüger N., Graichen, L., Hofmann-Winkler H., Kempf A., Winkler, M.S., Schulz S., Jäck H., Jahrsdörfer B., Schrezenmeier H., Müller M., Kleger A., Münch J., and Pöhlmann S., 2021, SARS-CoV-2 variants B.1.351 and P.1 escape from neutralizing antibodies, Cell, 184(9): 2384-2393.e12.
https://doi.org/10.1016/j.cell.2021.03.036
PMID: 33794143 PMCID: PMC7980144
Hossain M.K., Hassanzadeganroudsari M., and Apostolopoulos V., 2021, The emergence of new strains of SARS-CoV-2, what does it mean for COVID-19 vaccines?, Expert Review of Vaccines, 20(6): 635-638.
https://doi.org/10.1080/14760584.2021.1915140
PMID: 33896316 PMCID: PMC8074646
Kang C.Y., Chang S., Shin K.S., Jung I.K., Park H., Oh J., Park S., Shin J., and Kim J.H., 2023, Development of broadly protective COVID-19 vaccine against up-to-date variants based on adenovirus type 5/35 vector platform, The Journal of Immunology, 210(1_Supplement): 159-06.
https://doi.org/10.4049/jimmunol.210.supp.159.06
Lauring A.S., Tenforde M.W., Chappell J.D., Gaglani M., Ginde A.A., McNeal T., Ghamande S., Douin D.J., Talbot H.K., Casey J.D., Mohr N.M., Zepeski A., Shapiro N.I., Gibbs K.W., Files D.C., Hager D.N., Shehu A., Prekker M.E., Erickson H.L., Exline M.C., Gong M.N., Mohamed A., Johnson N.J., Srinivasan V., Steingrub J.S., Peltan I.D., Brown S.M., Martin E.T., Monto A.S., Khan A., Hough C.L., Busse L.W., Lohuis C.C.T., Duggal A., Wilson J.G., Gordon A.J., Qadir N., Chang S.Y., Mallow C., Rivas C., Babcock H.M., Kwon J.H., Halasa N., Grijalva C.G., Rice T.W., Stubblefield W.B., Baughman A., Womack K.N., Rhoads J.P., Lindsell C.J., Hart K.W., Zhu Y.W., Adams K., Schrag S.J., Olson S.M., Kobayashi M., Verani J., Patel M., Self W.H., and Influenza and Other Viruses in the Acutely Ill (IVY) Network 2022, Clinical severity of, and effectiveness of mRNA vaccines against, covid-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: prospective observational study, The BMJ, 376: e069761.
https://doi.org/10.1136/bmj-2021-069761
PMID: 35264324 PMCID: PMC8905308
Lazarević I., Pravica V., Miljanovic D., and Ćupić M., 2021, Immune evasion of SARS-CoV-2 emerging variants: what have we learnt so far?, Viruses, 13(7): 1192.
https://doi.org/10.3390/v13071192
PMID: 34206453 PMCID: PMC8310325
Li A.M., 2024, Technological innovation in disease detection and management in sugarcane planting, Bioscience Method, 15(1): 58-65.
https://doi.org/10.5376/bm.2024.15.0007
Menegale F., Manica M., Zardini A., Guzzetta G., Marziano V., d'Andrea V., Trentini F., Ajelli M., Poletti P., and Merler S., 2023, Evaluation of waning of SARS-CoV-2 vaccine-induced immunity: a systematic review and meta-analysis, JAMA Network Open, 6(5): e2310650.
https://doi.org/10.1001/jamanetworkopen.2023.10650
PMID: 37133863 PMCID: PMC10157431
Mohammed H., Pham-Tran D.D., Yeoh Z.Y.M., Wang B., McMillan M., Andraweera P.H., and Marshall H.S., 2023, A systematic review and meta-analysis on the real-world effectiveness of COVID-19 vaccines against infection, symptomatic and severe COVID-19 disease caused by the Omicron Variant (B.1.1.529), Vaccines, 11(2): 224.
https://doi.org/10.3390/vaccines11020224
PMID: 36851102 PMCID: PMC9965204
Mulligan M.J., Lyke K.E., Kitchin N., Absalon J., Gurtman A., Lockhart S., Neuzil K., Raabe V., Bailey R., Swanson K.A., Li P., Koury K., Kalina W., Cooper D., Fontes-Garfias C., Shi P.Y., Türeci Ö., Tompkins K.R., Walsh E.E., Frenck R., Falsey A.R., Dormitzer P.R., Gruber W.C., Şahin U., and Jansen K.U., 2020, Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults, Nature, 586(7830): 589-593.
https://doi.org/10.1038/s41586-020-2639-4
PMID: 32785213
Niyomnaitham S., Toh Z.Q., Wongprompitak P., Jansarikit L., Srisutthisamphan K., Sapsutthipas S., Jantraphakorn Y., Mingngamsup N., Licciardi P.V., and Chokephaibulkit K., 2022, Immunogenicity and reactogenicity against the SARS-CoV-2 variants following heterologous primary series involving CoronaVac, ChAdox1 nCov-19 and BNT162b2 plus BNT162b2 booster vaccination: an open-label randomized study in healthy Thai adults, Human Vaccines and Immunotherapeutics, 18(6): 2091865.
https://doi.org/10.1080/21645515.2022.2091865
PMID: 35816053 PMCID: PMC9746495
Notarte K.I., Guerrero-Arguero I., Velasco J., Ver A.T., de Oliveira M.H.S., Catahay J.A., Khan M.S.R., Pastrana A., Juszczyk G., Torrelles J.B., Lippi G., Martínez-Sobrido L., and Henry B.M., 2021, Characterization of the significant decline in humoral immune response six months post-SARS-CoV-2 mRNA vaccination: a systematic review, Journal of Medical Virology, 94(7): 2939-2961.
https://doi.org/10.1002/jmv.27688
PMID: 35229324 PMCID: PMC9088566
Paul P., El-Naas A., Hamad O., Salameh M.A., Mhaimeed N., Laswi I., Abdelati A.A., Alanni J., Khanjar B., Al-Ali D., Pillai K.V., Elshafeey A., Alroobi H., Burney Z., Mhaimeed O., Bhatti M., Sinha P., Almasri M., Aly A., Bshesh K., Chamseddine R., Khalil O., D’Souza A., Shree T., Mhaimeed N., Yagan L., and Zakaria D., 2023, Effectiveness of the pre-Omicron COVID-19 vaccines against omicron in reducing infection, hospitalization, severity, and mortality compared to delta and other variants: a systematic review, Human Vaccines and Immunotherapeutics, 19(1): 2167410.
https://doi.org/10.1080/21645515.2023.2167410
PMID: 36915960 PMCID: PMC10054360
Poh X.Y., Tan C.W., Lee I.R., Chavatte J.M., Fong S.W., Prince T., Hartley C., Yeoh A.Y.Y., Rao S., Chia P.Y., Ong S.W.X., Lee T.H., Sadarangani S.P., Lin R.J.H., Lim C., Teo J., Lim D.R.X., Chia W., Hiscox J.A., Ng L.F.P., Ren E.C,, Lin R.T.P., Rénia L., Lye D.C., Wang L.F., and Young B.E., 2022, Antibody response of heterologous vs homologous messenger RNA vaccine boosters against the severe acute respiratory syndrome coronavirus 2 omicron variant: interim results from the PRIBIVAC study, a randomized clinical trial, Clinical Infectious Diseases, 75(12): 2088-2096.
https://doi.org/10.1093/cid/ciac345
PMID: 35543372 PMCID: PMC9129205
Pratama N.R., Wafa I.A., Budi D.S., Sutanto H., Asmarawati T.P., Effendi G.B., and Wungu C.D.K., 2022, Effectiveness of COVID-19 vaccines against SARS-CoV-2 Omicron Variant (B.1.1.529): a systematic review with meta-analysis and meta-regression, Vaccines, 10(12): 2180.
https://doi.org/10.3390/vaccines10122180
PMID: 36560590 PMCID: PMC9783108
Rudan I., Adeloye D., and Sheikh A., 2022, COVID-19: vaccines, efficacy and effects on variants, Current Opinion in Pulmonary Medicine, 28: 180-191.
https://doi.org/10.1097/MCP.0000000000000868
Sharif N., Alzahrani K.J., Ahmed S.N., and Dey S.K., 2021, Efficacy, Immunogenicity and safety of COVID-19 vaccines: a systematic review and meta-analysis, Frontiers in Immunology, 12: 714170.
https://doi.org/10.3389/fimmu.2021.714170
Sun W.Q., He L.H., Zhang H., Tian X.D., Bai Z.H., Sun L., Yang L.M., Jia X.J., Bi Y.H., Luo T.R., Cheng G., Fan W.H., Liu W.J., and Li, J., 2021, The self-assembled nanoparticle-based trimeric RBD mRNA vaccine elicits robust and durable protective immunity against SARS-CoV-2 in mice, Signal Transduction and Targeted Therapy, 6(1): 340.
https://doi.org/10.1038/s41392-021-00750-w
PMID: 34504054 PMCID: PMC8426336
Tao K., Tzou P.L., Nouhin J., Gupta R.K., de Oliveira T., Pond S.L.K., Fera D., and Shafer R.W., 2021, The biological and clinical significance of emerging SARS-CoV-2 variants, Nature Reviews Genetics, 22(12): 757-773.
https://doi.org/10.1038/s41576-021-00408-x
PMID: 34535792 PMCID: PMC8447121
Thakur S., Sasi S., Pillai S.G., Nag A., Shukla D., Singhal R., Phalke S., and Velu G.S.K., 2022, SARS-CoV-2 mutations and their impact on diagnostics, therapeutics and vaccines, Frontiers in Medicine, 9: 815389.
https://doi.org/10.3389/fmed.2022.815389
PMID: 35273977 PMCID: PMC8902153
Thompson M.G., Burgess J.L., Naleway A.L., Tyner H.L., Yoon S.K., Meece J., Olsho L.E.W., Caban-Martinez A.J., Fowlkes A., Lutrick K., Kuntz J.L., Dunnigan K., Odean M.J., Hegmann K.T., Stefanski E., Edwards L.J., Schaefer-Solle N., Grant L., Ellingson K., Groom H.C., Zunie T., Thiese M.T., Ivacic L., Wesley M.G., Lamberte J.M., Sun X.X., Smith M.E., Phillips A.L., Groover K.D., Yoo Y.M., Gerald J., Brown R.T, Herring M.K., Joseph G., Beitel S., Morrill T.C., Mak J., Rivers P., Harris K.M., Hunt D.R., Arvay M.L., Kutty P., Fry A.M., and Gaglani M., 2021, Interim estimates of vaccine effectiveness of BNT162b2 and mRNA-1273 COVID-19 vaccines in preventing SARS-CoV-2 infection among health care personnel, first responders, and other essential and frontline workers-Eight U.S, Locations, December 2020-March 2021, Morbidity and Mortality Weekly Report, 70(13) 495-500.
https://doi.org/10.15585/mmwr.mm7013e3
PMID: 33793460 PMCID: PMC8022879
Wang P.F., Nair M.S., Liu L.H., Iketani S., Luo Y., Guo Y.C., Wang M., Yu J., Zhang B.S., Kwong P.D., Graham B.S., Mascola J.R., Chang J.Y., Yin M.T., Sobieszczyk M., Kyratsous C.A., Shapiro L., Sheng Z.Z., Huang Y.X., and Ho D.D., 2021, Antibody resistance of SARS-CoV-2 variants B.1.351 and B.1.1.7, Nature, 593(7857): 130-135.
https://doi.org/10.1038/s41586-021-03398-2
PMID: 33684923
Thompson M.G., Natarajan K., Irving S.A., Rowley E.A., Griggs E.P., Gaglani M., Klein N.P., Grannis S.J, DeSilva M., Stenehjem E., Reese S.E., Dickerson M., Naleway A.L., Han J., Konatham D., Mcevoy C., Rao S., Dixon B.E., Dascomb K., Lewis N., Levy M.E., Patel P., Liao I.C., Kharbanda A.B., Barron M.A., Fadel W.F., Grisel N., Goddard K., Yang D.H., Wondimu M.H., Murthy K., Valvi N.R., Arndorfer J., Fireman B., Dunne M.M., Embí P., Azziz-Baumgartner E., Zerbo O., Bozio C.H., Reynolds S., Ferdinands J., Williams J., Link-Gelles R., Schrag S.J., Verani J.R., Ball S., and Ong T.C., 2022, Effectiveness of a third dose of mRNA vaccines against COVID-19-associated emergency department and urgent care encounters and hospitalizations among adults during periods of delta and Omicron variant predominance-VISION network, 10 States, August 2021-January 2022, Morbidity and Mortality Weekly Report, 71(4): 139-145.
https://doi.org/10.15585/mmwr.mm7104e3
PMID: 35085224 PMCID: PMC9351525
Xu W., and Li J.H., 2024, Peptide-based vaccines for oral cancer: mechanisms of action and clinical outcomes, International Journal of Clinical Case Reports, 14(3): 132-143.
https://doi.org/10.5376/ijccr.2024.14.0015
Xu J.J., Lan X.Q., Zhang L.Y., Zhang X.J., Zhang J.Q., Song M.X., and Liu, J.Y., 2023, The effectiveness of the first dose COVID-19 booster vs full vaccination to prevent SARS-CoV-2 infection and severe COVID-19 clinical event: a meta-analysis and systematic review of longitudinal studies, Frontiers in Public Health, 11: 1165611.
https://doi.org/10.3389/fpubh.2023.1165611
PMID: 37325336 PMCID: PMC10267329
Zeng B.Q., Gao L., Zhou Q.X., Yu K., and Sun F., 2021, Effectiveness of COVID-19 vaccines against SARS-CoV-2 variants of concern: a systematic review and meta-analysis, BMC Medicine, 20(1): 200.
https://doi.org/10.1186/s12916-022-02397-y
PMID: 35606843 PMCID: PMC9126103
Zhang J., Yang W.X., Huang F.J., and Zhang K., 2023, Effectiveness of mRNA and viral-vector vaccines in epidemic period led by different SARS-CoV-2 variants: a systematic review and meta-analysis, Journal of Medical Virology, 95(3): e28623.
https://doi.org/10.1002/jmv.28623
PMID: 36852651

. FPDF(win)
. FPDF(mac)
. HTML
. Online fPDF
Associated material
. Readers' comments
Other articles by authors
. Tian Zhao
Related articles
. COVID-19 vaccines
. SARS-CoV-2 variants
. Vaccine efficacy
. Neutralization activity
. Immunogenicity
Tools
. Post a comment